












Dental Products
Patchogue Fluoride Treatment Dental Care: Stronger Teeth for Every Age
Patchogue fluoride treatment dental care matters because fluoride helps protect teeth before small weak spots…

Oral Care
Green Tea for Oral Health: A Simple Way to Support Your Smile
Green tea for oral health is a natural way to support your teeth and gums…
Oral Care
Oral Tie Release, What Parents Should Know Before and After Treatment
Oral tie release is a procedure used to free a tight band of tissue in…

Oral Care
Nature’s Smile Oral Rinse and Gum Balm: Oral Care Products With Natural Ingredients
Nature’s Smile Oral Rinse and Nature’s Smile Gum Balm are marketed as natural oral care…

Gum Disease
What to Do for Receding Gums at Home: Smart Steps That Help
Receding gums can be easy to miss at first. Maybe your teeth look a little…

Gum Disease
What to Use for Receding Gums: Best Options for Healthier Gums
Receding gums can be frustrating, uncomfortable, and a little scary when you first notice them.…
Gum Disease
Gum Disease From Dipping: How Smokeless Tobacco Harms Your Gums
Many people assume dipping is safer for the mouth than smoking. It is not. Smokeless…

Oral Care
Oral Surgery Aftercare Instructions: A Comprehensive Guide
Oral surgery after care instructions protect the blood clot, reduce bleeding, control pain, lower infection…

Dental Products
Dental Bone Loss Treatment: Best Options to Save Your Smile
Dental bone loss can sound alarming, but it is treatable in many cases. The key…
Gum Disease
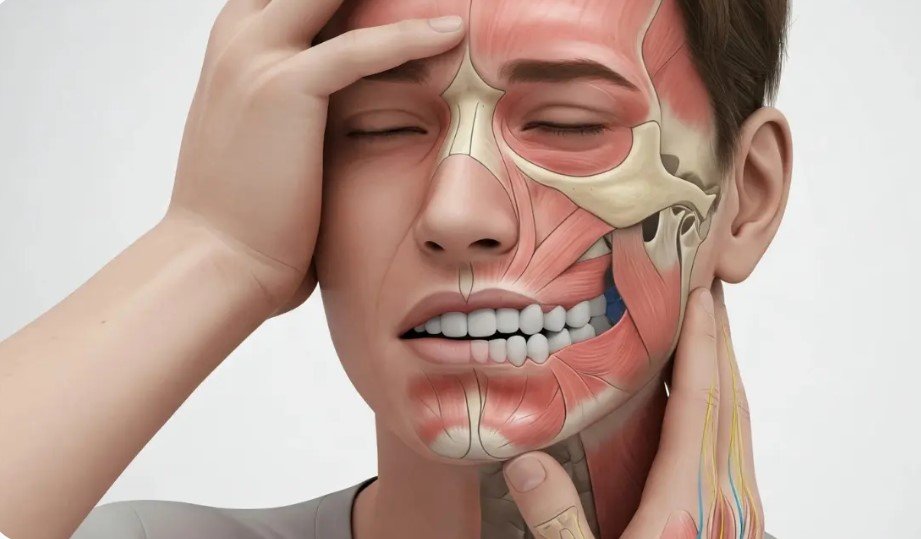
Gum Disease Headache: Can Unhealthy Gums Trigger Head Pain?
If you have sore gums and a nagging headache at the same time, it is…